
Types of Affect: A Practical Guide for Psychology and Mental Health Writing (With Examples)
Affect is one of the most important—and most misunderstood—concepts in clinical psychology and counseling. In everyday language, people use “mood” and “emotion” interchangeably. In professional settings, affect refers to the outward emotional presentation a clinician can observe. In other words, affect refers to the outward expression of emotion, including facial expression, tone of voice, gestures, posture, and the overall affect display a person shows during an interview.
This blog post explains the concept of affect, the dimensions of affect, and the different types of affect you will see in documentation, a mental status exam, or a mental status examination. You will also learn how affect appears in major mental disorders, including disorders such as schizophrenia, bipolar disorder, anxiety disorders, post-traumatic stress disorder, and neurological disorders (including brain injuries). Most importantly, you will get clear examples you can use in essays, case notes, and clinical discussions.
Affect in psychology: How mood and affect differ during a mental status examination
In affect in psychology, affect is typically defined as an observable emotional tone—what a person “projects” outward. Many clinicians write it exactly like this: affect refers to the patient’s visible emotional expression during the interaction.
- Mood and affect are related but different.
- Mood is the person’s sustained internal emotional state (“I feel depressed,” “I feel anxious”).
- Affect is the outward expression of that state (what the clinician sees and hears).
In a mental status examination, affect is documented because affect is often an immediate window into functioning. It can operate as affect as an indicator of acute distress, psychosis, mania, trauma activation, medication effects, or neurological change.
Example (documentation-style):
- Mood: “anxious.”
- Affect: “constricted, tense, appropriate to content.”
This distinction matters because a person can report one mood while showing a different affective presentation.
The dimensions of affect: A model of affect that explains “positive or negative” emotional patterns
Many frameworks describe the dimensions of affect using valence and activation:
- Valence: positive or negative (pleasant vs unpleasant).
- Activation: low vs high intensity (calm vs energized).
This is why you will often see “positive affect” and “negative affects” discussed together as positive and negative affect. In research, affect may be measured using the Positive and Negative Affect Schedule (often abbreviated as the positive and negative affect schedule, or PANAS). PANAS scores reflect how much a person is experiencing positive emotions (for example, enthusiasm, alertness) versus negative emotion (for example, distress, irritability).
Example (everyday):
- High activation + negative valence: panic, anger, agitation (a cluster of negative affective states).
- High activation + positive valence: excitement, motivation, joy (experiencing positive affect).
- Low activation + negative valence: sadness, fatigue, emptiness.
- Low activation + positive valence: calmness, contentment.
This “model of affect” is useful because it helps explain why two people can both feel “bad” but show different levels of energy and expression.
Various types of affect in clinical practice: main types clinicians describe in a mental status exam
Clinicians commonly document affect types by describing range, intensity, stability, and appropriateness. You will see statements such as “affect is characterized by…” because affect is not only what someone feels, but how it shows.
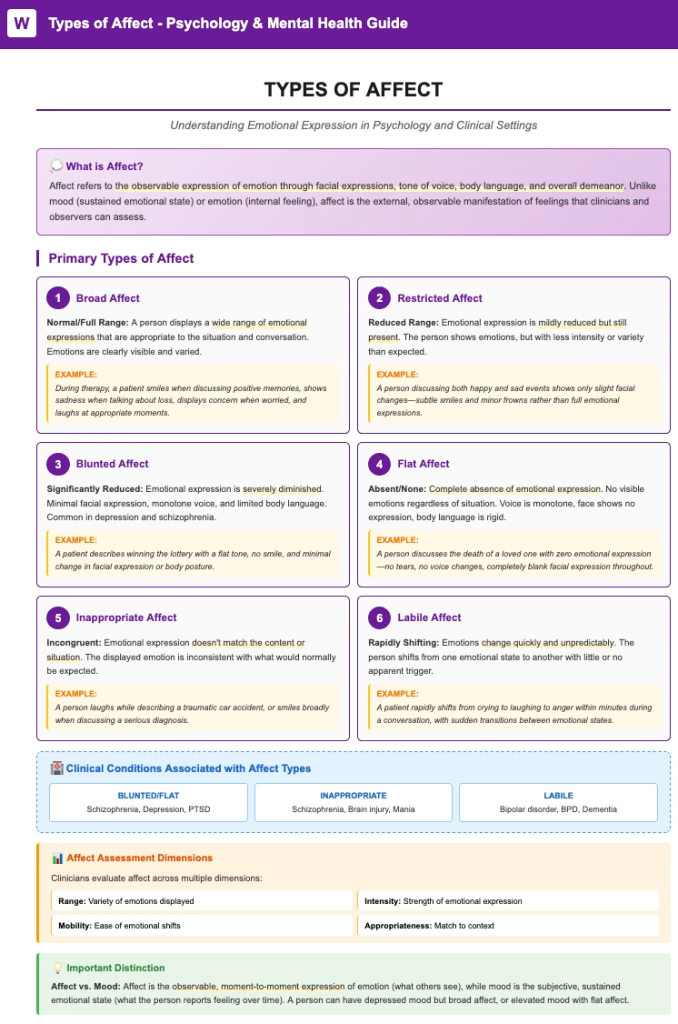
Below are the main types you will see in clinical writing. These are types of affect include (and many supervisors expect you to use these exact categories).
Broad affect: normal range and flexible emotional expression
Broad affect means the person’s affect has a full, normal range and shifts appropriately with discussion topics.
Example: Someone smiles when describing a positive event and becomes tearful when describing grief, with a matching emotional response.
Restricted affect and reduced affect: narrowed outward expression
Restricted affect describes limited range of affect; reduced affect is a similar phrase used when emotional expression is noticeably diminished.
Example: The person expresses emotion minimally even when content is highly emotional.
Constricted affect: Limited range but still reactive
Constricted affect is a mild-to-moderate narrowing—there is emotion, but it is muted or less varied.
Example: The person shows slight changes in facial expression but remains generally “tight” or controlled.
Labile affect: Rapid shifts in emotional state
Labile affect (sometimes written simply as labile) means affect changes quickly and unpredictably.
Example: Within minutes, the person laughs, then cries, then becomes angry without a clear stimulus.
This pattern is common in acute stress states and can occur in bipolar disorder or other mental health conditions.
Inappropriate affect: Mismatch with context
Inappropriate affect means the affect does not match the situation or content. Inappropriate affect may present as smiling while describing a traumatic death, or laughing during serious discussion.
Clinicians often explore the causes of inappropriate affect before assuming intent. Mismatch can reflect psychosis, neurological impairment, trauma responses, or social communication difficulty.
Blunted and flat affect: What they mean, how they appear, and why they matter
Two high-yield clinical terms are blunted affect and flat affect. Many learners confuse them.
Blunted affect: reduced emotional intensity
Blunted affect refers to significantly diminished emotional expression—emotion is present, but intensity is reduced.
- Blunted affect may look like limited facial movement, monotone speech, and minimal reactivity.
- A person with blunted affect may describe feelings internally, yet show little outward change.
- An individual with blunted affect may still respond slightly to humor or sadness, but the response is muted.
Example: “Patient reports sadness but shows minimal change in expression; voice remains monotone.”
Flat affect: near absence of outward emotional expression
Flat affect refers to an almost complete lack of visible emotion.
- A person with flat affect may show little to no facial expression, minimal gestures, and very limited changes in voice.
- People sometimes describe it as flat or blunted, but flat is usually more severe.
Example: “Patient’s face remains immobile; voice is monotone; minimal emotional response throughout interview.”
Flat affect in schizophrenia: a common documentation context
Flat affect in schizophrenia is commonly discussed because negative symptoms can include reduced emotional expressiveness. Clinicians may write affect in schizophrenia as flat or blunted, especially among patients with schizophrenia or people with schizophrenia who show negative symptom profiles. That said, affective presentation varies widely; not every person with schizophrenia has flat affect.
Causes of affect symptoms: when affect occurs in mental health conditions and neurological disorders
Affect is a symptom in many settings, but the causes differ. A careful note connects affect to the broader clinical picture, because affect involves brain function, stress physiology, learning history, and social context. In practice, affect shows up as part of the overall mental status picture.
Common contexts where affect changes:
Schizophrenia and psychotic-spectrum conditions
- Negative symptoms may include reduced expressiveness (flat or blunted).
- Disorganization can contribute to inappropriate affect.
Bipolar and mood disorder presentations
- In bipolar states, affect may be expansive, elevated, irritable, or labile affect may dominate.
- In a depressive episode, constricted or blunted affect is common.
These are often grouped under affective disorders and other mood disorder diagnoses.
Anxiety disorders and post-traumatic stress disorder
- Anxiety can narrow affect (constricted, tense) and amplify negative affect.
- Post-traumatic stress disorder may include emotional numbing (restricted affect) or sudden surges (labile affect), depending on triggers.
Personality disorder patterns
- Some personality disorder presentations include intense affect reactivity, unstable affect, or interpersonal affect shifts.
Brain injuries and neurological disorders
- Brain injuries can alter affect regulation, social perception, and expressive control.
- Some neurological disorders can lead to reduced facial mobility, monotone speech, or incongruent affect.
In all these cases, affect may shift based on medication, sleep, substance use, pain, or environmental stress. This is why careful observation and context matter.
Causes of inappropriate affect: Why mismatch can happen without “bad intent”
Clinicians are trained to explore reasons before judging. Causes of inappropriate affect may include:
- Psychosis or thought disorganization (especially in disorders such as schizophrenia)
- Neurological impairment affecting social cues
- Trauma responses (laughing as a defense)
- Severe anxiety (smiling to mask distress)
- Cultural communication differences
- Substance intoxication or withdrawal
- Emotional detachment due to chronic stress
In other words, the mismatch is not always deliberate. Often, it signals that underlying mental or neurological processes are shaping expression.
Affect refers to the outward expression of emotion: What mental health professionals observe
A mental health professional often documents affect by describing:
- Facial expression: mobile, reduced, immobile
- Tone of voice: monotone, pressured, animated, trembling
- Affect display: congruent or incongruent with content
- Outward expression of emotion: range and appropriateness
- Expression of emotion over time: stable vs labile
These observations help clarify whether a person can express emotion in ways that match their reported mood, environment, and narrative.
Positive affect and negative affects: Why they matter in research and treatment planning
Positive affect is not “happiness only.” It includes energy, engagement, interest, and motivation. Negative affects include distress, fear, hostility, guilt, and irritability.
Why does this matter?
- High negative affect is linked to risk for anxiety and mood symptoms.
- Low positive affect is commonly seen in depression and some trauma presentations.
- Tracking positive and negative affect can improve treatment targeting, especially when you use a structured tool like the Positive and Negative Affect Schedule (PANAS).
Example (clinical use): A therapist may track whether a client is experiencing positive affect more frequently after behavioral activation.
Want a clean, professor-ready MSE section that uses the right affect terms (without confusion)?
You will get:
A ready-to-paste MSE affect paragraph (accurate, concise, and clinically worded)
Correct examples and definitions matched to your course expectations
Optional full Mental Status Examination write-up with strong structure and formatting support
Affect as an indicator: When affect can help guide diagnosis and risk assessment
Because affect is observable, it often guides decision-making:
- Affect can help identify acute risk (severe agitation, intense despair, emotional shutdown).
- It can support diagnostic differentiation (for example, mania vs anxiety vs trauma activation).
- It can show treatment response (increased range, improved regulation, better congruence).
However, clinicians must avoid overinterpretation. A flat presentation can reflect depression, medication, cultural style, dissociation, or neurological limitation. That is why affect is interpreted alongside thought process, perception, cognition, and functioning.
Treat flat and blunted affect: What helps depends on the cause
Treatment is diagnosis-driven. There is no single approach that fits every case of reduced expression.
When flat or blunted affect is linked to psychosis-spectrum conditions
- Treatment may include antipsychotic medication management (medical scope) and psychosocial rehabilitation.
- Skills-focused interventions may support emotional communication and social functioning.
When reduced affect is linked to depression, trauma, or anxiety
- Cognitive behavioral therapy can target avoidance, negative beliefs, and behavioral withdrawal.
- Behavioral therapy approaches (including behavioral activation) can increase engagement and opportunities for positive emotion.
- Trauma-focused therapy can reduce numbing and improve affective range when appropriate.
When brain injuries or neurological disorders contribute
- Rehabilitation, speech-language therapy, and neuropsychological interventions may be needed.
- Environmental supports can improve affect regulation and communication.
If your assignment requires a phrase like treat flat, you can write: “To treat flat or reduced affect, clinicians target the underlying condition, strengthen affect regulation skills, and support behavioral engagement.”
Real-world examples: Different types of affect in short clinical-style vignettes
- Broad affect:
A client smiles when describing a promotion and becomes tearful when discussing a loss, with congruent tone and expression. - Constricted affect:
A client reports feeling sad, shows limited facial movement, but becomes visibly tense discussing triggers. - Restricted affect:
A client talks about painful events with minimal outward emotion and limited changes in voice. - Blunted affect:
A client reports grief but shows muted emotional expression; voice remains monotone; slight reaction appears with probing. - Flat affect:
A client maintains an immobile face and monotone voice across all topics, including intensely emotional content. - Labile affect:
A client rapidly shifts from laughter to tears to anger with minimal external stimulus. - Inappropriate affect:
A client laughs while describing a serious assault; on exploration, they report feeling numb and disconnected.
Final takeaway: Types of affect include observable patterns, not stereotypes
Affect is central to clinical assessment because it bridges inner experience and outward behavior. Affect occurs across many mental health conditions and health condition contexts, and it can shift with setting, stress, medication, and neurological status. The key is accurate description, context, and ethical interpretation.
Need an essay-ready section or a full paper?
If you are writing a psychology assignment, counseling case analysis, or mental status examination write-up, IvyResearchWriters.com can help you produce clear, correct, high-scoring work.
Visit IvyResearchWriters.com and message: “AFFECT WRITE-UP” to get:
- A rubric-aligned outline and draft
- Correct definitions and clinical examples
- Polished formatting (American Psychological Association or your required style)
- Clean, original writing you can paste directly into your document
Frequently Asked Questions
1) What are the nine affects?
There are different “lists” depending on the model you are using, but a widely taught framework in psychology is Silvan Tomkins’ nine innate affects. In this model, affect plays a core role in motivation and how humans respond to cues, and emotions can affect attention, learning, and behavior.
The nine affects (Tomkins):
- Interest–Excitement
- Enjoyment–Joy
- Surprise–Startle
- Distress–Anguish
- Fear–Terror
- Anger–Rage
- Shame–Humiliation
- Disgust
- Dissmell (an aversive response to bad odors, distinct from disgust)
Why this matters clinically: Affect is not only “how someone looks.” It connects to drive, avoidance, social connection, and coping—so affect also influences how symptoms present in interviews and therapy.
2) What are examples of affect?
Affect is the observable emotional expression. In practice, affect often shows up in facial expression, tone, and overall responsiveness. Here are clear examples you can use in assignments:
Examples (short, documentation-style):
- “Affect euthymic and congruent with stated mood.”
- “Affect anxious; tearful at times; appropriate to content.”
- “Affect irritable; tense posture; clipped responses.”
- “Affect labile with rapid shifts from laughter to tears.”
- “Affect blunted with limited reactivity.”
- “Affect flat with minimal facial movement and monotone speech.”
One key clarification: An individual can report sadness but show limited outward emotion. That does not automatically mean dishonesty—affect would be interpreted alongside the full clinical picture (thought process, cognition, context, and medication effects).
3) What are the 7 types of emotions?
People use “types of emotions” in different ways. If you need a clean, commonly accepted set for coursework, you can use a basic “core emotions” list. These help explain why emotions can affect behavior and decision-making (for example, fear driving avoidance, anger driving confrontation).
A practical 7-emotion list (commonly taught):
- Happiness/Joy
- Sadness
- Fear
- Anger
- Disgust
- Surprise
- Contempt (sometimes included as a core social emotion in expanded models)
If your instructor prefers a different model (for example, Ekman’s commonly taught “basic emotions”), IvyResearchWriters.com can tailor the exact list to match your course expectations.
4) What are the different types of affect in MSE?
In the Mental Status Examination (MSE), clinicians document “types of affect” by describing range, intensity, stability, and appropriateness. This is one reason affect plays a major role in the MSE: it provides observable data about emotional functioning.
Common affect descriptors used in MSE:
- Broad (full range)
- Constricted (limited range but still reactive)
- Restricted (more limited range)
- Blunted (markedly reduced intensity)
- Flat (near-absent emotional expression; includes experiencing flat presentation outwardly)
- Labile (rapid shifts)
- Inappropriate (mismatch with context/content)
- Congruent vs incongruent with mood/content
- Euthymic (neutral/steady, often documented when stable)
How to write it well: Affect in an MSE is best documented with 2–3 descriptors, for example:
- “Affect constricted, anxious, congruent with content.”
- “Affect blunted, minimally reactive, mood incongruent at times.”